When the Immune System Targets Your Hair
What Is It?
Alopecia areata is an autoimmune condition in which the body’s immune system mistakenly attacks hair follicles, resulting in sudden, non-scarring hair loss. It often shows up as smooth, round bald patches on the scalp or beard—but can affect any hair-bearing area.
Prevalence
- Affects about 2% of the population
- Occurs equally in men and women
- The most common form of alopecia diagnosed in children
- More than 70% experience the onset of the condition before the age of 40, and early onset is often associated with a more severe disease course 1
- In some cases, the condition progresses to more severe forms:
- Around 5% of patients experience complete scalp hair loss (alopecia totalis)
- 1% of patients develop total loss of body hair (alopecia universalis)
Why It Happens
While the exact cause is unknown, alopecia areata likely results from a combination of:
- Genetic predisposition (15% have a family history)
- Weakened immune system
- Physical or emotional stress
- Illness or viral infections
- Hormonal changes (pregnancy, menopause, postpartum)
- Nutritional deficiencies
- Autoimmune Conditions (thyroid, lupus, rheumatoid arthritis)
Types of Alopecia Areata
Alopecia Areata | Alopecia Barbae
Well-defined, round, or oval bald patches on the scalp or other parts of the body characterize the most common form of autoimmune hair loss. The bald patches are smooth, without scarring, and may involve a single or multiple patches.
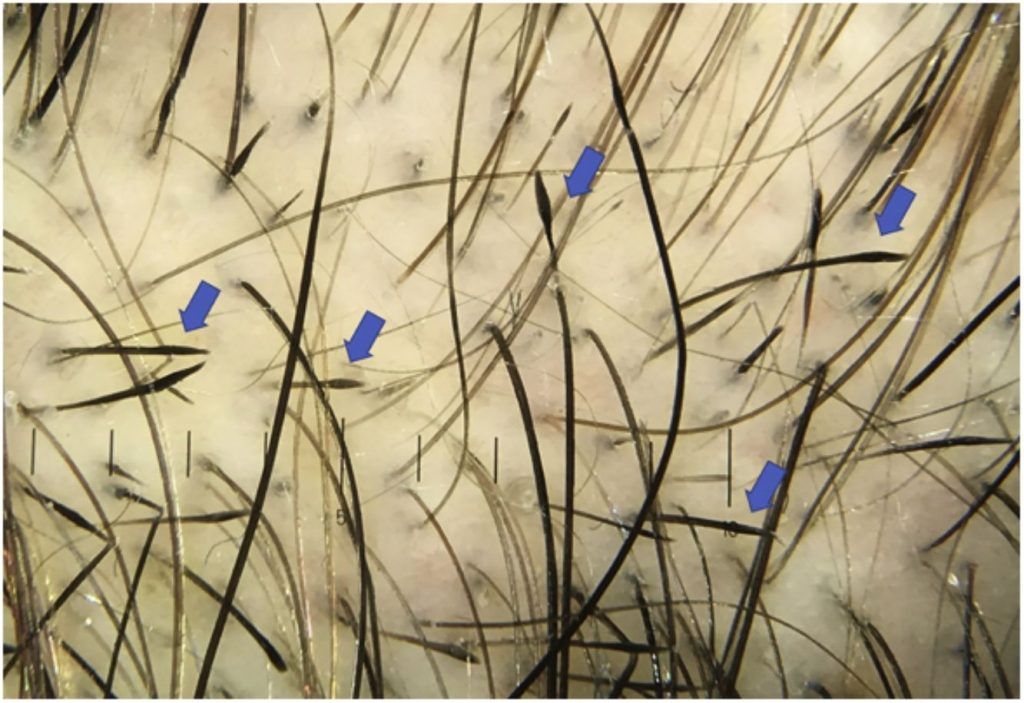

Trichoscopy typically shows yellow dots, black dots, exclamation mark hairs, and broken hairs, which reflect active follicle attack, along with vellus hairs in regrowth.



Alopecia Totalis
This is a more severe form of alopecia areata, involving complete hair loss on the scalp. It often begins as patchy hair loss that progresses to total scalp hair loss. Eyebrow and eyelash loss may also be involved.

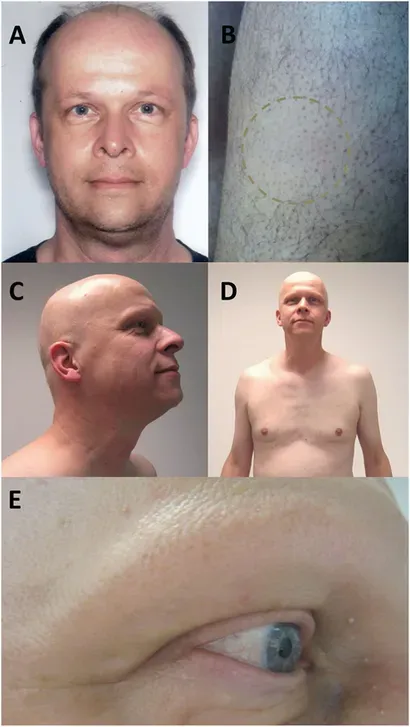
Alopecia Universalis
This is the most extensive form of alopecia areata, characterized by complete hair loss on the scalp, face (including eyebrows and eyelashes), and body (including pubic and underarm hair).
Diffuse Alopecia Areata and Alopecia Areata Incognita
The two most common variants of non-patchy AA are alopecia areata incognita (AAI) and diffuse alopecia areata (DAA). Hair loss is generalized in these variants, with no clear bald patches.
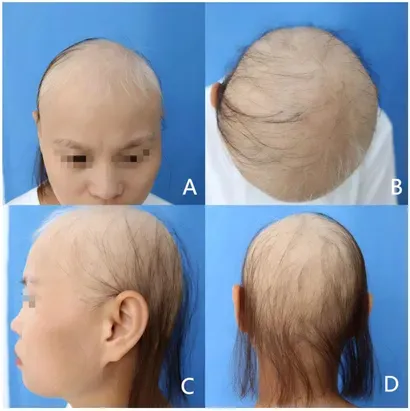
Diffuse alopecia areata is a less common subtype characterized by widespread hair thinning across the scalp, predominantly affecting the hairline and temples rather than distinct patches. Hair shedding occurs suddenly, often leading to a significant reduction in hair density within a short time frame, but not as rapidly as alopecia areata incognita.
Alopecia areata incognita is another condition characterized by widespread and rapid hair shedding, often occurring along the occipital (back of the scalp) and parietal regions (sides and top of the scalp), and typically develops within a few weeks.
Diffuse Alopecia Areata
Alopecia Areata Incognita


A high percentage of these patients are also affected by androgenetic alopecia. They both often resemble telogen effluvium or androgenetic alopecia in appearance, making it more challenging to diagnose. As a result, a scalp biopsy may be needed in uncertain cases to confirm the diagnosis and distinguish it from telogen effluvium or androgenetic alopecia.
Ophiasis Pattern
This form of alopecia areata has a specific pattern of hair loss, characterized by bald patches that form at the nape of the neck and extend toward the temples.
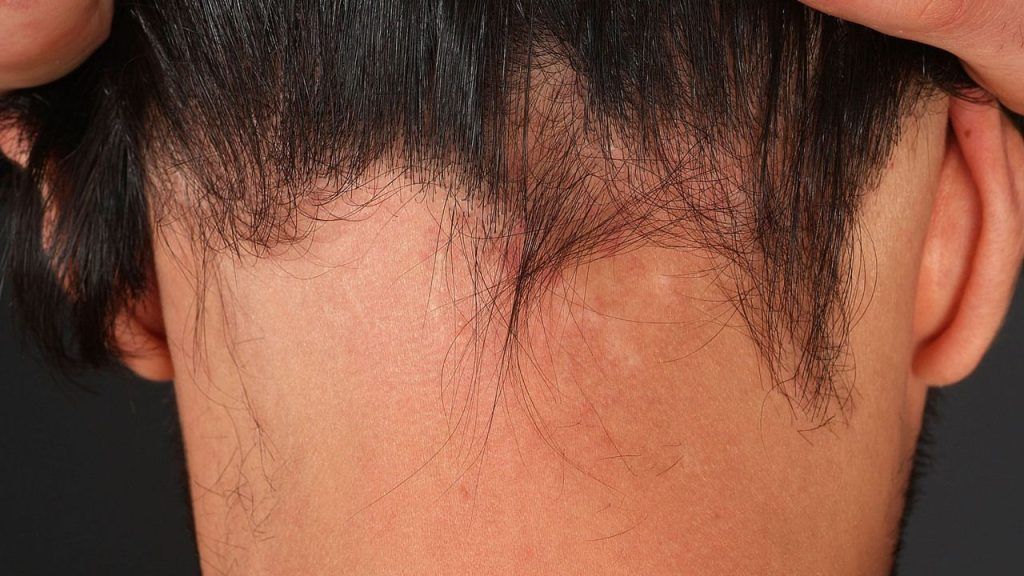
This subtype is more challenging to treat than other forms of alopecia areata and is frequently resistant to standard treatments.
Diagnosis
Because some types mimic other conditions like androgenetic alopecia (AGA) or telogen effluvium, diagnosis may include:
- Scalp & hair exam
- Medical History
- Blood tests (may be ordered to rule out other conditions that can cause hair loss)
- Scalp biopsy (if unclear or to rule out other conditions)
Treatment Options
A consultation with a dermatologist ensures that the condition is managed effectively and that the underlying causes are addressed.
- Topical/injected steroids – Reduce inflammation
- Topical immunotherapy – Create a mild allergic reaction to re-stimulate growth
- Oral JAK inhibitors – Target immune pathways in extensive cases
- Minoxidil (off-label) – Aids regrowth in mild/moderate cases (response rate ~60%)
- Stress management – Reduces flares in stress-sensitive patients
- Hair transplant – Not recommended unless the condition has been inactive for 2+ years
Prognosis
The prognosis of alopecia areata is unpredictable, with spontaneous regrowth occurring in some individuals within a few months, while others may experience persistent or recurrent hair loss.
Some individuals may not respond to treatment, and others may progress to more severe forms of alopecia areata, such as alopecia totalis or alopecia universalis. Early diagnosis and treatment improve outcomes and reduce the risk of progression.
While some individuals may experience a single episode, others may face recurrent or prolonged episodes of hair loss throughout their lives.

