What Is Female Pattern Hair Loss?
Androgenetic alopecia, also known as female pattern hair loss (FPHL), is the most common cause of hair loss in women—accounting for nearly half of all cases.
Hair Loss Goes Beyond the Scalp
Hair is more than just appearance—it’s tied to confidence, identity, and femininity. For many women, especially during and after menopause, hair thinning can feel like losing a part of themselves. This emotional weight is often made worse by the beauty industry’s constant marketing of quick-fix treatments—most of which are more hype than science.
Early Signs Can Be Easy to Miss
FPHL doesn’t always show up the way you might expect. Initially, it may appear to be just extra hair shedding or a slightly wider part. Because of this, it’s often mistaken for temporary, stress-related hair loss. Unfortunately, this can delay proper treatment and allow the condition to progress.
That’s why it’s so important to be evaluated by a hair loss specialist. They can help you pinpoint the actual cause(s) and create a treatment plan that actually works.
How Common Is Hair Loss? The Numbers May Surprise You
Female pattern hair loss is common in the United States, affecting over 30 million women. Its likelihood increases with age and can vary based on race. While FPHL is less common than male pattern baldness, it often has a greater emotional and psychological impact on women. This is mainly due to societal expectations and the emphasis on hair as a key part of appearance and identity, making hair loss a particularly sensitive issue for many women.
Prevalence of Female Pattern Hair Loss by Age:
- Puberty to age 29: 12%
- Ages 30 to 49: 25%
- Ages 50 to 69: 41%
- Ages 70 and up: >50%
- Only 43% of women > 80 years old show no evidence of FPHL
Hair Loss Across Ethnicities
Hair isn’t just a reflection of your health—it’s part of your identity. But did you know hair loss can present differently depending on your background?
Ethnicity & Female Pattern Hair Loss (FPHL)
| Ethnic Group | Estimated Prevalence | Key Insights |
|---|---|---|
| Caucasian Women | 30–35% | FPHL is most common in this group. |
| Asian Women | 5–10% | Rates increase with age, but still lower than in Caucasians. |
| African American Women | 8–15% | Often mixed with other hair-loss types like traction alopecia. |
| Indian & Middle Eastern Women | 20–30% | Similar rates to Caucasians, influenced by regional and genetic factors. |
| Hispanic/Latina Women | ~25–30% | Comparable to Caucasian rates, but can vary widely. |
What Causes Female Pattern Hair Loss?
AGA is a complex condition caused by the interaction of genetic, hormonal, environmental, and lifestyle factors.
Genetic Influence
FPHL isn’t caused by a single gene—it’s polygenic. That means multiple genes from both sides of your family play a role in determining your risk. You might inherit one gene from your mother, another from your father, and a few others that silently influence how your hair behaves over time.
Genetic variations can cause hair loss to:
- Skip generations
- Affect the age of onset, speed, and severity
- Show up differently even among siblings
So, even if no one in your immediate family shows signs of thinning, that doesn’t mean you’re in the clear. Between 15% and 30% of women with female pattern hair loss do not have a strong family history of hair loss. The genetic blueprint can skip generations or show up in different ways—like early thinning, more shedding, or changes in hair texture.
Think of it like this: Your DNA holds a deck of cards. The more hair loss-related genes you’re dealt, the greater your chance of developing FPHL. But genes are just one part of the equation—lifestyle, hormones, nutrition, and stress also matter.
Genetic variations can cause hair loss to:
- Skip generations
- Show up differently even among siblings
- Affect the age of onset, speed, and severity
Therefore, while hair loss tends to run in families, it does not always do so in a predictable manner. It’s also possible to develop AGA without a strong family history—genes from other chromosomes and subtle environmental influences still play a role.
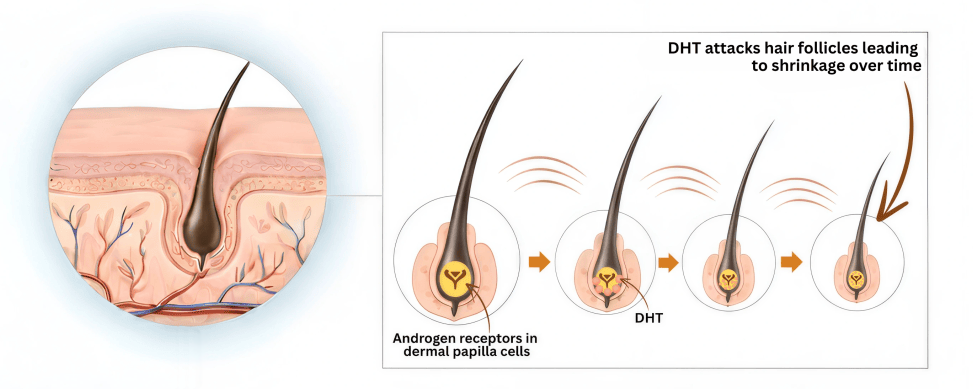
Hormonal Sensitivity to DHT
AGA is strongly linked to DHT (dihydrotestosterone), a byproduct of free testosterone that attacks hair follicles in genetically sensitive individuals. It’s made when an enzyme called 5-alpha reductase converts free testosterone into a more potent form. While DHT is often discussed in male hair loss, it also affects women—just more subtly and unpredictably.
DHT plays a key role in male development, but it isn’t a key hormone for women. It’s made in small amounts and doesn’t play a role in female development. Instead, estrogen and progesterone are the main drivers behind breast development, periods, and fertility. However, when DHT levels rise too high in women, it often causes problems like hair thinning, acne, or unwanted facial or body hair.
Like in men, DHT attaches to receptors in genetically sensitive hair follicles, especially around the crown, temples, and part line. Over time, it shrinks these follicles, causing:
- Thinner, finer, less pigmented hairs
- Nearly invisible hairs (vellus)
- Shorter hair growth cycles
- Excess shedding
- Difficulty regrowing lost hair
This process is known as miniaturization—and it’s the hallmark of female pattern hair loss (FPHL).
Over time, thick, pigmented hairs, known as terminal hairs, are replaced by thin, light-colored, nearly invisible hairs called vellus hairs. This transformation occurs due to a gradual shortening of the hair cycle’s growth phase (the anagen phase) and the lengthening of the resting phase (telogen phase). As the condition progresses, the hair becomes finer, less pigmented, and sparser, resulting in noticeable thinning.
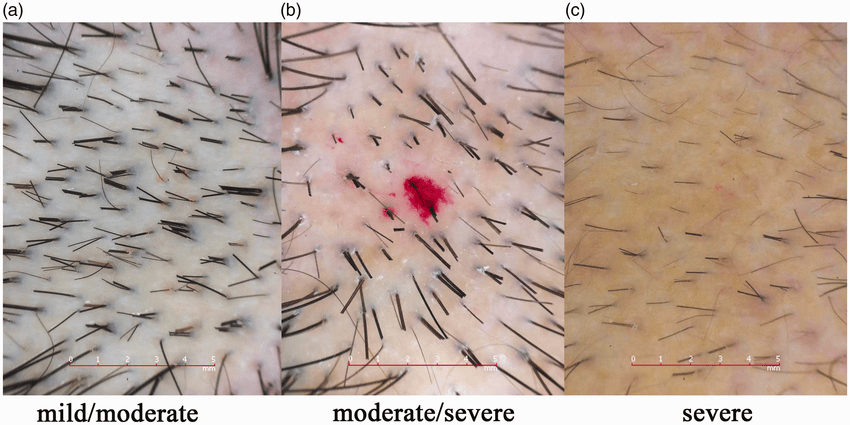
Trichoscopy shows variation in hair shaft diameters, more miniaturized/vellus hairs, peripilar halos, and reduced follicular density, which together confirm patterned hair thinning.
In women, hair follicle miniaturization tends to be less uniform and less severe than in men. As a result, women typically do not experience completely bald areas on the scalp, except in very rare cases.
While this gradual thinning or miniaturization is common, some individuals may also experience periods of increased shedding. The extent and severity of hair loss vary between individuals and are primarily determined by genetic factors.
Do DHT Levels Determine Your Hair’s Fate?
A common assumption is that “if DHT causes hair loss, shouldn’t we test for it?”
It’s a fair question, but the answer isn’t so simple.
Why Blood DHT Doesn’t Tell the Full Story:
- DHT levels in your scalp are what matter, not your blood 1
- You can have “normal” blood DHT but still have high levels in your scalp
- Some people have high DHT and no hair loss — their follicles don’t mind it because they have reduced sensitivity
Most women with DHT-related hair loss have completely normal testosterone levels.
What this comes down to is your genetic sensitivity to DHT, and not the amount of DHT you produce. However, if you are sensitive to DHT, the more you make, the more hair loss you may have.
The issue isn’t how much testosterone you make—it’s how your hair follicles respond to it. Unlike men, where DHT is a clear culprit, fewer than 15% of women with FPHL have high androgen (e.g., DHT) blood levels. Still, scalp-level DHT sensitivity can cause follicles to shrink.
You might have:
- More 5-alpha reductase activity (producing more DHT)
- More DHT receptors in your hair follicles
- A stronger genetic sensitivity to DHT
- Variations in enzyme and receptor activity—like different levels of 5α-reductase, aromatase, and androgen receptors.
What Increases DHT in Women?
Several factors can boost DHT activity or sensitivity:
- Genetic predisposition
- Menopause (due to a drop in protective estrogen)
- High-androgen birth control pills or IUDs
- Testosterone therapy (even when “bioidentical”)
- PCOS (Polycystic Ovarian Syndrome)
Signs Your Hair Loss May Be DHT-Driven
- Family history of hair thinning (on either side)
- Gradual thinning, especially at the midpart line or crown
- More scalp showing through your hair
- Hair feels less dense, or ponytail is smaller
- No itching, redness, or inflammation
DHT may be a “male hormone,” but it absolutely impacts women too—especially when it comes to hair health. Understanding how it works is the first step toward finding the right treatment plan tailored to your biology and goals.
Age & Menopause
As women age, estrogen levels naturally decline—especially during and after menopause. Since estrogen helps protect hair follicles, this drop can make hair thinning more noticeable. That’s why female pattern hair loss tends to become more common with age.
Lifestyle & Environmental Factors
You may carry the genes, but environmental factors, hormones, and stress can influence when, where, and how fast hair loss shows up.
Click here to understand more about epigenetics and how it can impact your hair loss and treatment response.
Why It’s Complicated
Hair loss is a personal, complex, and often misunderstood issue. It’s not just about aging or your parents’ hairlines. It’s about the unique interaction between your genes, hormones, health, and environment. The good news? With the proper evaluation, there are effective ways to manage, slow, and in some cases reverse hair loss.
Early diagnosis leads to better results. If you’re noticing changes in your hair, it’s worth taking a closer look.
Mapping the Stages of Hair Loss
Female pattern hair loss (FPHL) typically presents in one of two ways. The most common is gradual thinning across the top of the scalp—especially along the middle part—while the hairline stays mostly intact. This type of thinning can be hard to notice at first, but over time, it becomes more obvious when styling or parting the hair. Doctors use a few different scales to assess how far the hair loss has progressed.
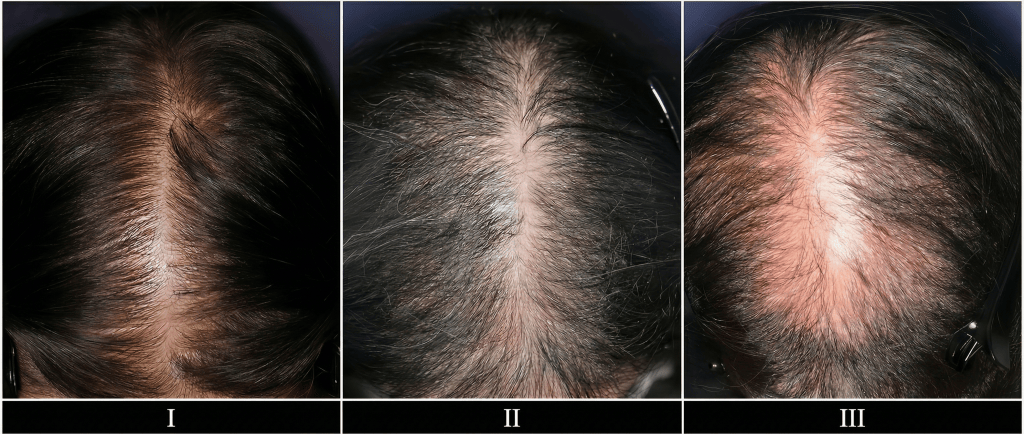
The Ludwig Scale: A Crown-Based Grading System
The Ludwig scale focuses on how much hair is thinning at the crown (top) of the scalp. It breaks hair loss down into three stages:
- Stage I – Mild Thinning. Slight widening of the midpart line, but hair still looks full overall. The hairline stays intact.
- Stage II – Moderate Thinning. Thinning becomes more visible, and the scalp starts to peek through. Styling gets harder because of volume loss.
- Stage III – Advanced Thinning. Hair is very thin, especially down the middle of the scalp. It becomes difficult to hide the thinning, even with styling.
The Sinclair Scale: A Simple Way to Track Female Hair Thinning
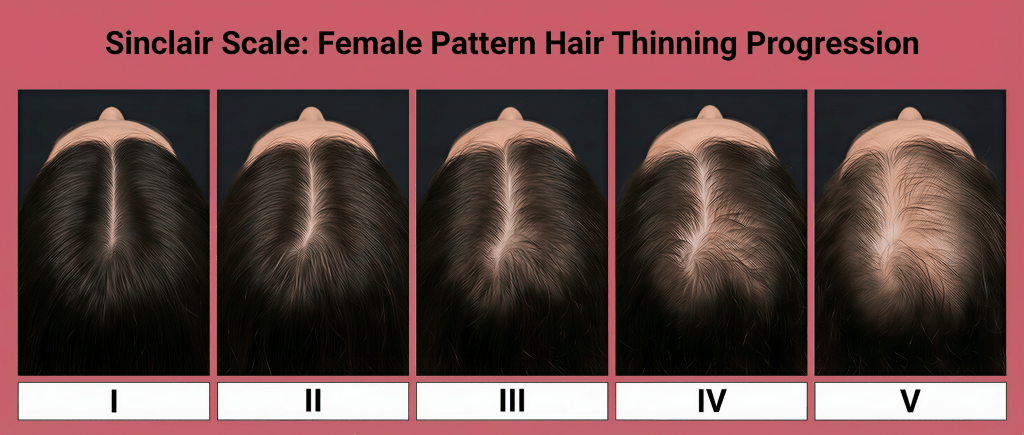
The Sinclair scale ranges from Grade 1 (normal density used as the baseline for comparison) to Grade 5 (advanced thinning). It focuses on how much the midpart line has widened and the extent of overall thinning present. Because it’s simple, this scale is preferred in everyday practice—it’s intuitive and easy for both doctors and patients to rate themselves.
The Olsen Scale: The “Christmas Tree” Pattern
Some women lose hair in a specific pattern where thinning starts at the midscalp and spreads out toward the front hairline. This creates a triangle-shaped area that looks like a Christmas tree.
This scale is the most common type of hair loss seen in women—especially those with early or mild thinning. Around 70% of affected women show this pattern.


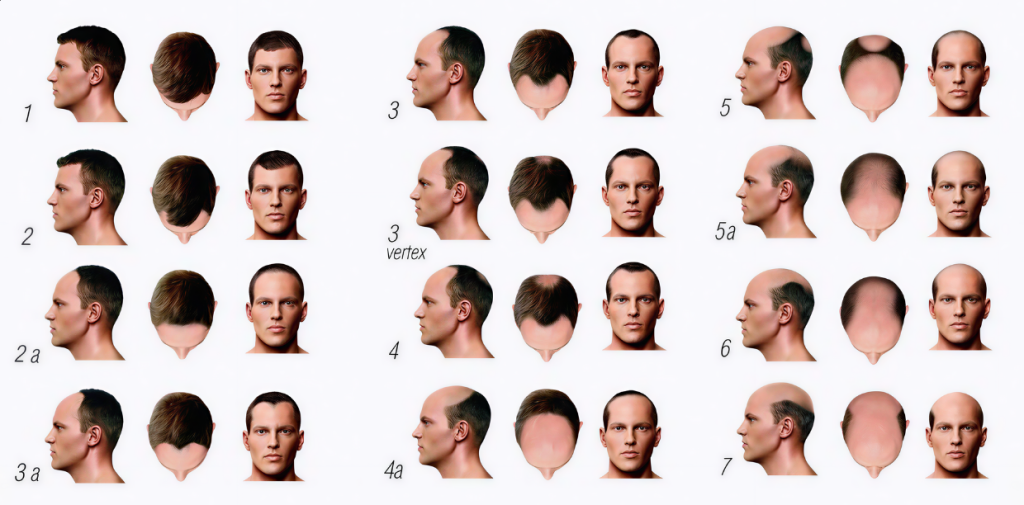
The Hamilton-Norwood Pattern: More Common After Menopause
Although usually seen in men, this pattern of hair loss can show up in women—especially after menopause or in women with high androgen levels. It’s marked by a receding hairline and thinning at the crown.
Roughly 37% of postmenopausal women may develop this pattern. It’s also more likely in women using testosterone. This further highlights the hormonal and age-related factors that contribute to hair loss.
Hair Loss Along the Back of the Scalp: What You Need to Know
Why the Back of the Scalp Usually Stays Full in Men
In men, hair loss typically skips the back of the scalp—the occipital region. That’s because these follicles have fewer DHT hormone receptors. It’s like having a protective shield that stops thinning—and that shield makes occipital hair perfect for transplanting elsewhere.

Women: A Different Hair Loss Pattern
Surprisingly, about one-third of women with female pattern hair loss (FPHL) also experience thinning at the back of the scalp, below the crown. When this happens, the extent often matches the front hair loss. Why?
- Genetically susceptible to losing hair everywhere
- Non-hormonal triggers—stress, nutrient deficiencies, autoimmune issues, or lifestyle factors—can affect hair beyond androgen (DHT) sensitivity
- These androgen-independent factors can leave the occipital area just as vulnerable
When the back thins out, it points to deeper, more complex causes.
Why the Occipital Region Matters in Treatment
Doctors count on the back of the head for hair transplants—hair is safest there. But when occipital hair thins:
- Donor strength is weakened, reducing surgery success
- Planning must shift to only medical therapies that can stabilize or regrow hair naturally
- A 360° evaluation (full review of history, lifestyle, scalp exam, and labs)
What You Can Do Next
- Ask your specialist to include the back of the scalp in every exam
- Explore treatments like minoxidil, low level laser, or PRP that support all affected areas
- Dive deeper into possible nutrient or stress factors that could be weakening your follicles on multiple fronts
Hair loss at the back of the scalp isn’t just cosmetic—it’s a sign that the usual approach may not be enough. A personalized, full-spectrum treatment plan that addresses both hormones and other root causes is key to strong, stable results.
Curious if your occipital hair is safe— or what treatment mix is right for you? Book a consultation for a comprehensive evaluation.
Diagnosing Hair Loss: It’s More Than Just Looking at Your Scalp
Hair loss is often more complex than it appears, especially in women, which often requires more in-depth investigation than men, as multiple factors can contribute to their hair loss. Additionally, more than one type of hair loss may occur simultaneously.
At YAKER Hair Restoration + Med Spa, we don’t just treat symptoms — we find the why.
A 360-Degree Approach
A proper evaluation includes:
- Hair loss history: timeline and pattern of hair loss
- AI-powered scalp analysis with TrichoLab for precise imaging
- Review of hair loss history
- Review of medical & family history
- Review of medications, supplements, nutrition, hair care products and practices
- Lifestyle factors (stress, sleep, etc.)
- Comprehensive blood testing
What If It’s Not Genetic Hair Loss?
Not all hair loss is caused by genetics. When there’s sudden, patchy, or widespread shedding, we dig deeper.
Other causes we consider:
- Telogen effluvium (TE): Triggered by stress, illness, nutritional or hormonal imbalances, and scalp or systemic inflammation
- Diffuse alopecia areata: Autoimmune-related hair loss
- Cicatricial (scarring) alopecia: Inflammation that permanently damages hair follicles
These conditions often overlap, making it difficult to determine what is truly happening. That’s why a thorough evaluation matters.
When women notice thinning hair, it’s often a sign of more than hair issues—it can hint at deeper health changes. Let’s explore the hidden causes—and what you can do about them.
What’s Happening Inside: Hidden Health Links to Hair Loss
When most people think of hair loss, they assume it’s only a cosmetic issue. But androgenetic alopecia (AGA)—also known as female pattern baldness—is more than a hair issue. Research shows it can be connected to other health problems that share similar genetic, hormonal, or metabolic roots.
Polycystic Ovary Syndrome (PCOS) & Hair Loss
What Is PCOS?
PCOS affects 6–10% of premenopausal women and is one of the most common causes of infertility.
One of the most common medical conditions linked to female pattern hair loss (FPHL) is polycystic ovarian syndrome (PCOS). In fact, one study in over 4,000 women showed that up to 91% of women with PCOS also experience FPHL. That’s because PCOS can raise levels of male hormones like testosterone and DHEA-S, which fuel the miniaturization of hair follicles.
Why PCOS Causes Hair Loss
Think of hair follicles as delicate plants in a garden. Hormonal imbalances—with too much testosterone—send out signals that stress the roots. For women with PCOS, increased testosterone (and its byproduct DHT) shrinks hair follicles, leading to noticeable thinning.
How PCOS Affects Your Health
- Irregular cycles
- Skin issues like cystic acne
- Fertility challenges
- Weight gain
- Unwanted facial or body hair
- Risk of type 2 diabetes, high blood pressure, high cholesterol, heart disease, sleep apnea
- Delayed diagnosis—sometimes over a decade
Birth control pills often hide these symptoms (irregular periods, acne, unwanted hair growth), which means PCOS can stay undetected until birth control is stopped. Additionally, the lack of education and accessible resources about PCOS often leads to confusion and improper management of the condition.
PCOS & Testosterone Use
Some hormone clinics prescribe testosterone for fatigue or other complaints—but this can backfire. Too much testosterone boosts DHT, which can trigger hair loss in women with a genetic predisposition. Notably:
- Free testosterone converts to DHT and directly affects follicles
- Many women on testosterone therapy have levels 2–15 times higher than normal and are not monitored properly
What You Can Do
Talk to your OBGYN
If you have irregular periods, acne, unwanted facial or body hair, and hair thinning
Balance hormone treatment
Combine lifestyle changes with medications like anti-androgens or birth control that regulate androgen levels. Avoid testosterone therapy given your susceptibility to hair loss.
Protect your hair follicles
Treat hair loss early with therapies like minoxidil and finasteride/dutasteride (if applicable).
PCOS is a powerful influencer of hair loss—due to its link with higher testosterone. Untamed hormone therapy can worsen hair loss if you’re genetically prone. A thoughtful, balanced approach, with monitoring and professional guidance, is the best way to protect your hair and overall well-being.
Metabolic Syndrome
Metabolic syndrome is another health condition that often goes hand-in-hand with hair loss.2 It includes a combination of issues like insulin resistance, belly fat, high blood pressure, low “good” cholesterol (HDL), and high triglycerides. One study found that nearly half of women with FPHL also had metabolic syndrome, and others show a higher risk of heart disease in these women. 3
Other Associations
Hair loss is also a window into nutrient status. A large study showed that the most common conditions associated with FPHL were:
- Nutrient deficiencies (83.9%)
- Autoimmune disease (14.8%)
- Psychological stress (12.3%)
- Thyroid disorder (7.7%)
Of the nutrient deficiencies, the top 3 were:
- Iron deficiency (70.3%)
- Zinc deficiency (39.4%)
- Combined iron and zinc deficiency (25.8%)
These findings show that thinning hair is often more than a cosmetic issue—it can reflect underlying health issues.
What Makes Female Pattern Baldness Worse?
Female pattern hair loss (FPHL) often occurs alongside other health issues that quietly influence how and why hair starts to thin.
Beyond short-term triggers, ongoing health conditions also play a role that puts stress on the hair cycle.
Some of these conditions can also push more hair into the shedding phase, leading to telogen effluvium. That’s why a full evaluation is key to uncovering and addressing the root cause of hair loss—not just the symptoms.
Birth Control and Hair Loss: What You Should Know
Combination birth control pills contain synthetic forms of estrogen (ethinyl estradiol) and progesterone (progestin). While these hormones are commonly used to regulate periods, prevent pregnancy, and treat acne, some types can quietly trigger or worsen hair loss.
There are two main ways this happens:
- Genetic Hair Loss Activation or Acceleration – Birth control can speed up hair thinning in women who are genetically predisposed to female pattern hair loss (FPHL)
- Telogen Effluvium (Shedding) – Some women experience temporary, increased shedding due to hormonal shifts when starting or stopping birth control
Not all birth control pills are created equal. The key difference lies in the type of progestin they contain. Unlike natural progesterone, progestins in many pills have androgenic activity, meaning they act like testosterone. This can increase DHT levels—the hormone that shrinks hair follicles in women with a genetic sensitivity. Pills with a high progestin-to-estrogen ratio are more likely to cause thinning.
On the other hand, pills with higher estrogen levels (around 30 micrograms of ethinyl estradiol) and low-androgen index progestins may actually help support hair growth by prolonging the growth (anagen) phase of the hair cycle.
Most combination pills contain 10 to 35 micrograms of this synthetic estrogen. For example, Lo Loestrin Fe has only 10 micrograms of estrogen—too little to offset the effects of progestin in women vulnerable to hair loss.
Low-Androgen Index Birth Control Pills
| Progestin Type | Brand name |
| Desogestrel-Ethinyl Estradiol | Desogen, Reclipsen, Orthocept |
| Drospirenone-Ethinyl Estradiol | Yasmin, Yaz |
| Norethindrone | Ortho Micronor, Nor-QD, Aygestin, Lyza |
| Norethindrone-Ethinyl Estradiol | Ovcon-35, Brevicon, Modicon, Ortho-Novum 7/7/7, Tri-Norinyl |
| Norgestimate-Ethinyl Estradiol | Ortho-Cyclen, Ortho Tri-Cyclen |
High-Androgen Index Birth Control Pills
| Progestin Type | Brand name |
| Levonorgestrel-Ethinyl Estradiol | Seasonale, Seasonique, Aviane, Portia, Levora |
| Norgestrel-Ethinyl Estradiol | Lo/Ovral, Cryselle, Low-Ogestrel |
| Ethynodiol Diacetate-Ethinyl Estradiol | Demulen 1/35, Zovia 1/35 |
| Norethindrone Acetate-Ethinyl Estradiol | Loestrin, Microgestin, Junel, Estrostep |
While birth control pills with the strongest progestins include levonorgestrel and norgestrel, the combination of an ample amount of estrogen with these progestins lowers the medication’s overall androgenic potential.
If your hair loss began after starting or stopping birth control, it’s worth talking to your doctor about switching to a hormone combination that’s gentler on your hair.
Progestin-Based IUDs
Progestin-based intrauterine devices (IUDs) are a popular form of long-term, reversible birth control placed in the uterus. They are also commonly used to reduce heavy menstrual bleeding and cramping, and are a good option for individuals who cannot take estrogen.
Unlike copper IUDs, they release a synthetic hormone of progesterone (progestin) called levonorgestrel. Unlike natural progesterone, progestins have androgenic activity, a synthetic hormone that can increase levels of testosterone and its byproduct, DHT, the main driver of genetic hair loss. Those with a genetic sensitivity to DHT may notice gradual thinning over time.
Think of DHT like a “shrinking signal” to your hair follicles. If you’re already sensitive to that signal, certain birth control pills can speed up the miniaturization process—causing the hairs to become finer, shorter, and eventually stop growing altogether.
Common levonorgestrel IUDs include:
| Progestin-Based IUD | Levonorgestrel Dosage |
| Mirena | 52 mg |
| Liletta | 52 mg |
| Kyleena | 19.5 mg |
| Skyla | 13.5 mg |
Non-Hormonal IUD: Paragard
Paragard is a copper IUD that prevents pregnancy through copper’s natural sperm-repelling properties—it does not contain hormones and does not stop ovulation. Women often choose it to avoid hormonal side effects.
Why It Matters for Hair
If you’ve experienced hair loss or shedding while on hormonal birth control, talk with your OBGYN about switching from a higher-androgen hormonal IUD to one with a lower androgen index progestin, if hormonal methods are still needed.
Menopause, Hysterectomy & Hair
Life events that alter hormonal balance—like menopause or a hysterectomy—can influence hair health. Here’s how:
- Estrogen drops → Estrogen shields hair follicles and helps with moisture. Without it, hair can feel dry, brittle, and more prone to breakage and hair loss
- Progesterone declines → Progesterone (not progestin) helps block testosterone from turning into DHT. As levels fall, hair becomes more sensitive to androgens
- Androgen effect increases → Even if testosterone doesn’t rise, its negative effects on hair grow stronger when estrogen and progesterone fall, promoting hair thinning
It’s common for women to notice more noticeable hair thinning or changes in hair texture during this phase.
Testosterone Therapy: A Double-Edged Sword
Finding the Right Balance: Why Testosterone Levels Matter for Women
Testosterone therapy is growing in popularity among women—often marketed to boost energy, mood, libido, and muscle tone. But more testosterone isn’t always better. For women, the key is balance, not excess.
Free vs. Total Testosterone: Know the Difference
Free testosterone is the active form your body uses to regulate libido, muscle growth, mood—and yes, hair loss.
It’s also the form that gets converted into DHT, the main driver of AGA.
Too many clinics focus on total testosterone levels without ever measuring free testosterone, which is what really matters when it comes to treating low testosterone and hair loss risk.
How DHT Sensitivity Accelerates Hair Loss
Everyone makes DHT, but not everyone’s hair reacts the same.
- If you’re genetically sensitive, even normal levels of DHT can trigger hair loss
- If you’re not genetically sensitive, you might have high testosterone and still keep your hair
The key isn’t just how much testosterone you have—it’s how your follicles respond to it. That’s why pushing testosterone too high (even for “anti-aging” reasons) can speed up hair loss in vulnerable patients.
Optimal Testosterone Levels by Age
With the growing popularity of testosterone replacement therapy (TRT), I regularly see women seeking help for hair loss concerns. Alarmingly, 90% of these patients have testosterone levels well above the normal range for their age. More than 65% do not have their hormone levels monitored regularly, and 95% fail to test free testosterone.
In women, testosterone levels peak in their early 20s.
- Late teens to early 20s: Highest average levels
- After mid-20s: Levels gradually decline with age
- By menopause: Testosterone levels drop by about 50% from peak values
All testosterone values can vary slightly between laboratories, but here’s a general guide:
| Age | Total T (ng/dL) | Free T |
|---|---|---|
| 19–49 | 15–70 | 0.02–0.50 ng/dL (0.2–5 pg/mL) |
| 50+ | 5–45 | 0.01–0.35 ng/dL (0.1–3.5 pg/mL) |
Aim to keep your free testosterone in the average range for your age—not above it. Ensure labs include free testosterone, not just total levels.
Going too high cannot only increase your chances of experiencing more hair loss but also lead to other unwanted side effects.
The Dark Side of High Testosterone: What Every Woman Should Know
When testosterone levels climb too high—especially without proper monitoring—it can lead to serious, sometimes irreversible side effects.
Hormonal & Reproductive Disruptions
- Irregular or missed periods
- Infertility (from ovulation suppression)
- Breast swelling or tenderness
Signs of Virilization (Male-Like Changes)
- Deepening of the voice (may be permanent)
- Unwanted facial and body hair growth
- Clitoral enlargement at excessively high levels (often irreversible)
Heart & Metabolic Risk
- Polycythemia → thickened blood, leading to blood clot, heart attack, and stroke risk
- Increased LDL, decreased HDL → heart disease
- Insulin resistance → poor blood sugar control→ higher chance of developing type 2 diabetes
Liver & Kidney Strain
- Potential liver toxicity and impaired kidney function
Mood & Behavior
- Heightened aggression or irritability
- Mood swings
- Anxiety or depressive symptoms
Skin & Hair
- Oily skin and acne breakouts
- Accelerated hair loss in genetically prone individuals
- Increased DHT levels, which can worsen seborrheic dermatitis due to excess scalp oil and inflammation
Can Testosterone Trigger Hair Loss—Even with Using Hair Treatments?
Yes—and here’s why.
If you’re using DHT blockers (like finasteride/dutasteride) but still losing hair on testosterone, this might explain it:
Think of it like blood pressure meds—you can’t eat high-sodium foods and expect the pill to work.
Similarly, if you’re increasing DHT with high testosterone, it can overpower the meds trying to reduce it.
Why Hormone Clinics Often Miss the Hair-Loss Connection
When you see a hormone specialist to optimize your testosterone, hair loss may not even come up. That’s because:
Genetics Aren’t on Their Radar
Hormone doctors focus on lab numbers—not hair loss history. But if you have the genes for female pattern hair loss, your follicles react more strongly to DHT (a byproduct of testosterone).
Final Thoughts on Testosterone
If you’re concerned about hair loss while on testosterone therapy:
- Let your hormone specialist know about your hair loss
- Stay within age-appropriate ranges—provide your free testosterone range to your hormone specialist to ensure they don’t go too high
- Get your free testosterone checked regularly—not just total testosterone
- Avoid chain clinics that follow a one-size-fits-all approach
- Combine therapy with proper DHT-blocking treatments (if applicable)
Insulin Resistance and Hair Loss
Insulin resistance or diabetes can worsen genetic hair loss by:
- Increasing free testosterone → more DHT conversion
- Reducing blood flow to the scalp → fewer nutrients to the hair follicles
- Promoting inflammation and oxidative stress → damaged hair follicles
The fix: Control blood sugar, improve circulation, reduce inflammation, and address hormone balance.
The Smart Way to Approach Hair Loss Treatment
Treating AGA effectively means looking at the whole picture—including your hair loss history, health, genetics, and lifestyle.
These details help build the most effective strategy for slowing or stopping the loss and improving hair density.
What Actually Works?
Currently, topical minoxidil is the only FDA-approved treatment for female pattern hair loss. But even then, only about 40% of users see significant improvement when it’s used as the sole therapy.
Other Promising Off-Label Treatments Include:
- Oral or topical Finasteride or dutasteride (if applicable)
- Oral minoxidil
- Spironolactone
- Low level laser therapy (LLLT)
- Platelet rich plasma (PRP) injections
- Nutritional optimization
These therapies can help slow the progression of hair loss and improve hair thickness. However, they cannot regrow hair in fully bald areas, and results are not permanent—if you stop treatment, most gains fade within 6–12 months.
Why Starting Early Matters
AGA is a progressive condition, meaning it gets worse with age. Once hair follicles miniaturize beyond a certain point, they become unresponsive—even to the best treatments.
- Start early
- Stay consistent
- Pair medical and lifestyle interventions
- Consider comprehensive lab testing and evaluation
Ready to explore personalized options? Explore your treatment options here.

