Commonly referred to as male pattern baldness (MPB), it is the most common cause of hair loss in men, accounting for 95% of cases. It affects up to 80% of men at some point and can start as early as the early to late teens.
The prevalence of male pattern baldness in the United States is extensive, affecting approximately 50 million men in the population. Most studies suggest that the incidence increases steadily with age, and without treatment, hair density (fullness) decreases by approximately 6% per year.
A common misconception is that hair thinning and baldness are simply a result of aging. While hair can naturally thin mildly as we age, significant hairline recession or noticeable hair loss that leads to scalp visibility is typically a sign of androgenetic alopecia.
How Common Is Hair Loss? The Numbers May Surprise You
Hair loss becomes more common as men age, following this general pattern:
- 20s: 20%
- 30s: 30%
- 40s: 40%
- 50s: 50%
- 70s: up to 80%
The condition typically follows a predictable pattern, characterized by a receding hairline, thinning crown, or both. Some men lose their hair quickly, while others experience gradual hair loss over several decades.
Hair Loss Across Ethnicities
Hair isn’t just a reflection of your health—it’s part of your identity. But hair loss doesn’t affect everyone the same way. Your background can influence how, when, and even where you lose hair. Understanding these differences can help you better recognize what’s normal, what’s not, and when to seek help.
Ethnic Differences in Male Pattern Hair Loss
Caucasian Men
Highest prevalence of androgenetic alopecia (male pattern baldness), often beginning in their 20s or 30s.
African American Men
About 4 times less likely to develop pattern baldness compared to Caucasian men. When hair loss occurs, it often progresses more slowly.
Asian Men
Around 1.5 times less likely to experience pattern baldness than Caucasian men. They tend to have more diffuse thinning rather than receding hairlines.
Middle Eastern and Indian Men
Fall somewhere between Asian and Caucasian men in terms of prevalence. The onset and pattern of thinning vary, but crown thinning is more common than receding temples.
Recognizing how hair loss presents across different ethnic backgrounds can help you avoid misdiagnosis and choose the right treatment path early on. If you’re noticing changes in your hair, no matter your background, don’t wait to speak with a hair loss specialist.
What Causes Male Pattern Hair Loss?
AGA is a complex condition caused by the interaction of genetic, hormonal, environmental, and lifestyle factors.
Genetic Influence
AGA isn’t caused by a single gene—it’s polygenic. That means multiple genes from both sides of your family play a role in determining your risk. A common myth is that it only comes from your mom’s side. This misinterpretation stems from a study conducted in 1916. While the androgen receptor (AR) gene is located on the X chromosome (inherited from the mother), studies show that over 80% of men with balding also have a father with hair loss. Additionally, AGA is inherited through recessive genes, meaning two copies—one from each parent—are typically needed for the trait to manifest. However, the interaction between these multiple genes can increase or decrease the chances of hair loss in complex ways.
Genetic variations can cause hair loss to:
- Skip generations
- Affect the age of onset, speed, and severity
- Show up differently even among siblings
Therefore, while hair loss tends to run in families, it does not always do so in a predictable manner. It’s also possible to develop AGA without a strong family history—genes from other chromosomes and subtle environmental influences still play a role.
Hormonal Sensitivity to DHT
AGA is strongly linked to DHT (dihydrotestosterone), a byproduct of free testosterone that attacks hair follicles in genetically sensitive individuals.
DHT is a hormone that plays a key role in male development during puberty. It helps form the male genitalia, increases muscle mass, deepens the voice, and stimulates body and facial hair growth.
But in adulthood, DHT’s role shifts—and not in a good way. While it’s no longer essential after puberty, DHT contributes to several issues:
- Hair Loss (Androgenetic Alopecia): DHT shrinks hair follicles over time, leading to thinning and balding.
- Oily Skin and Acne: DHT increases sebum production, which clogs pores and fuels acne breakouts.
- Seborrheic Dermatitis: By promoting excess oil production, DHT can worsen scalp inflammation and flaking associated with seborrheic dermatitis.
- Benign Prostatic Hyperplasia (BPH): DHT stimulates the growth of the prostate gland, which can lead to urinary symptoms like urgency, a weak stream, or incomplete emptying in older men.
The DHT-Hair Loss Connection
An enzyme called 5α-reductase converts free testosterone into DHT, which then binds to androgen receptors in genetically susceptible hair follicles. Interestingly, total testosterone levels are generally similar in men with and without androgenetic alopecia (AGA). However, individuals with AGA tend to have higher levels of free testosterone, the active form of the hormone, which contributes to the increased production of DHT.
This interaction causes the hair follicles to shrink, resulting in thinner hair and, ultimately, hair loss. This process is known as miniaturization—and it’s the hallmark of male pattern baldness.
Over time, thick, pigmented hairs, known as terminal hairs, are replaced by thin, light-colored, nearly invisible hairs called vellus hairs. This transformation occurs due to a gradual shortening of the hair cycle’s growth phase (the anagen phase) and the lengthening of the resting phase (telogen phase). As the condition progresses, the hair becomes finer, less pigmented, and sparser, resulting in noticeable thinning.
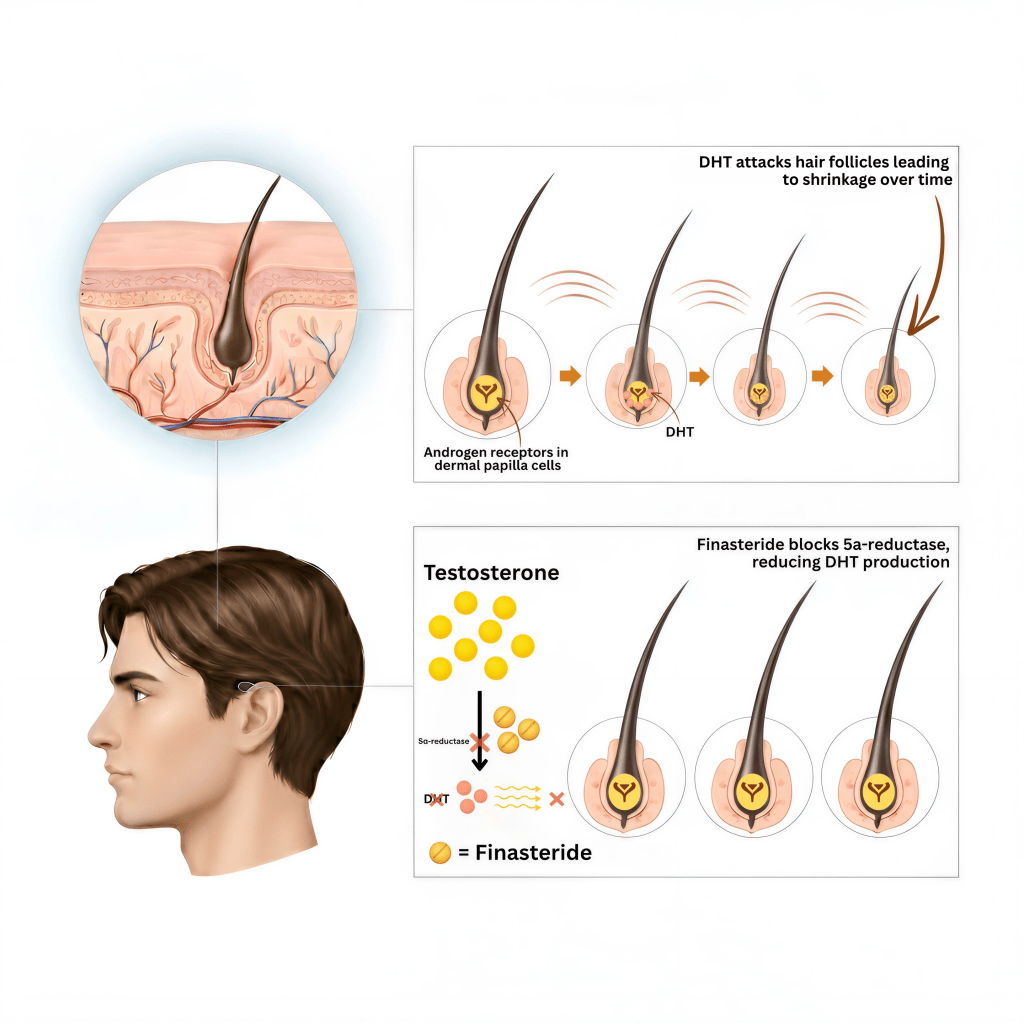
The hair follicles in the hairline, frontal area, and crown are more susceptible because they have higher concentrations of DHT, 5α-reductase enzyme, and androgen receptors, particularly in individuals with AGA. The level of androgen receptors is 1.5 times higher in the frontal scalp compared to the back and sides of the scalp, below the crown. Since hair follicles along the back and sides of the scalp have fewer receptors for the DHT hormone to attach to, hairs from this area are primarily used in hair transplantation procedures.
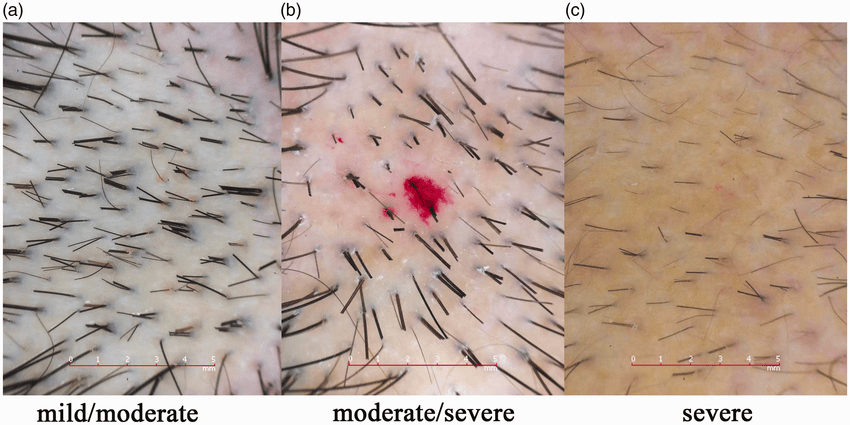
Trichoscopy shows variation in hair shaft diameters, more miniaturized/vellus hairs, peripilar halos, and reduced follicular density, which together confirm patterned hair thinning.
While this gradual thinning or miniaturization is common, some individuals may also experience periods of increased shedding. The extent and severity of hair loss vary between individuals and are primarily determined by genetic factors.
Eventually, this process can lead to baldness, as the affected follicles stop producing visible hair, and the pores where hair normally grows are smoothed over with skin.
In the mid-to-late stages of hair follicle miniaturization, a condition called perifollicular fibrosis—the buildup of scar-like tissue around the hair follicles—is often observed. This can make it harder for treatments for androgenetic alopecia (AGA) to work effectively.
Do DHT Levels Determine Your Hair’s Fate?
A common assumption is that “if DHT causes hair loss, shouldn’t we test for it?”
It’s a fair question, but the answer isn’t so simple.
- Total DHT (blood test)
- Measures the overall amount of DHT in the blood (both bound + free)
- ~98–99% is bound to proteins (mainly SHBG, some albumin)
- Bound DHT isn’t directly active but serves as a reservoir
- Free DHT (blood test):
- Measures the small fraction of unbound DHT circulating in your bloodstream
- Tells you how much biologically active DHT is available systemically
- It does not directly reflect how much DHT is acting in a specific tissue, like the scalp
Why Blood DHT Doesn’t Tell the Full Story
- DHT levels in your scalp are what matter, not your blood 1
- You can have “normal” blood DHT but still have high levels in your scalp
- Some people have high DHT and no hair loss — their follicles don’t mind it because they have reduced sensitivity
Scalp DHT (tissue level)
- Refers to the local concentration of DHT inside the scalp/hair follicles
- This is where DHT binds androgen receptors and drives hair follicle miniaturization in androgenetic alopecia
- Scalp levels can be very different from blood levels, since DHT is produced locally in hair follicles by 5-alpha reductase activity
How Scalp DHT Can Be Measured
- Requires a scalp biopsy (removing a small piece of scalp skin)
- The tissue is then analyzed in a research lab for intrafollicular DHT levels
- Sometimes measured in clinical trials studying finasteride/dutasteride but not offered in standard labs
Why It’s Not Done in Practice
- Invasive, uncomfortable, leaves a scar
- Costly and not covered by insurance
- No validated commercial test exists
- Results wouldn’t typically change treatment, since we already know DHT in the scalp drives androgenetic alopecia and we target it with standard medications
What this comes down to is your genetic sensitivity to DHT, and not the amount of DHT you produce. However, if you are sensitive to DHT, the more you make, the more hair loss you may have.
This study supports that conclusion. Researchers compared DHT levels in people with and without hair loss and found that the levels were about the same in both groups. This suggests that simply having more DHT in your system isn’t what causes hair loss. Instead, the key factor seems to be how sensitive your hair follicles are to DHT. Some people’s follicles are genetically more responsive to it, which can trigger hair thinning—even if their hormone levels are completely normal.
Lifestyle & Environmental Factors
You may carry the genes, but medical conditions, nutrition, lifestyle, and environmental factors can influence when, where, and how fast hair loss shows up.
Click here to understand more about epigenetics and how it can impact your hair loss and treatment response.
Why It’s Complicated
Hair loss is a personal, complex, and often misunderstood issue. It’s not just about aging or your parents’ hairlines. It’s about the unique interaction between your genes, hormones, health, and environment. The good news? With proper evaluation, effective ways exist to manage, slow, and in some cases reverse hair loss.
Early diagnosis and treatment lead to better results. If you’re noticing changes to your hair, it’s worth taking a closer look.
Mapping the Stages of Hair Loss
Hair loss typically follows a predictable pattern. It often begins with hair loss at the temples and a receding hairline at the front, forming an “M” shape. Thinning at the crown (vertex) is common and may gradually spread forward, resulting in more noticeable hair loss over time.
Hamilton-Norwood Scale: A Roadmap for Male Hair Loss
The Hamilton-Norwood scale is a tool used to track the stages of male pattern baldness. Think of it as a map that shows how hair loss progresses over time. It’s divided into seven stages, starting with a slight recession of the hairline and ending with extensive balding across the top of the scalp.
Doctors and hair specialists use this scale to understand where someone is in their hair loss journey.
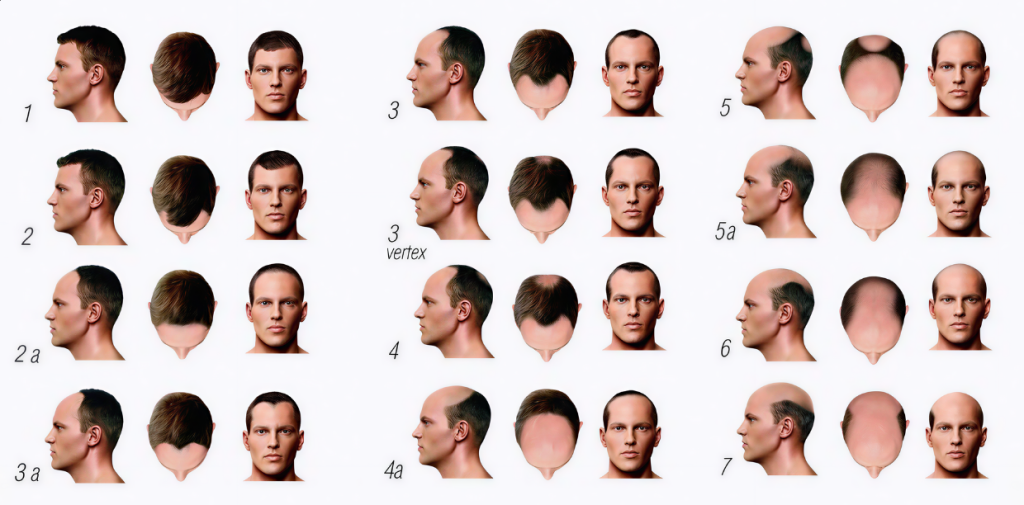
Stage 1:
- No significant hair loss
- The hairline appears full with no noticeable recession
Stage 2:
- Slight recession at the temples (often called a “mature hairline”)
- Still looks natural, but the corners of the hairline begin to move back
Stage 3:
- The first stage that is considered true balding
- Deeper recession at the temples forming an “M” shape
- May also see early thinning at the crown (NW 3V)
Stage 4:
- More severe temple recession and a visible bald spot at the crown
- A band of hair along the midscalp still separates the front hairline from the crown
Stage 5:
- Hair loss at the front and crown is more significant
- The band of hair along the midscalp becomes thinner and narrower
Stage 6:
- The bridge of hair along the midscalp disappears
- The bald areas at the front and crown merge into a larger bald area
- The band of hair along the back and sides of the scalp (“horseshoe pattern”) remains
Stage 7:
- Most severe stage of hair loss
- The band of hair along the sides and back becomes much thinner and lower
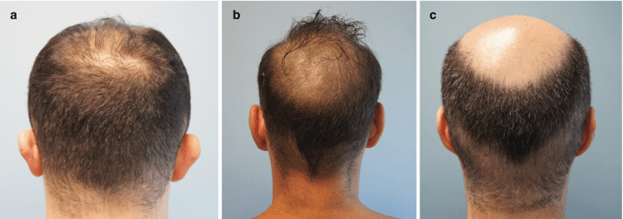
What Is Retrograde Alopecia?
Retrograde alopecia (RA) is a type of hair loss that often co-occurs with hereditary hair loss. It begins at the nape of the neck and progresses upward, affecting areas typically resistant to hair loss. It can also affect the hair along the temples.
- Often seen in advanced stages of hair loss
- It can limit the availability of donor hair for hair transplantation
- It is important to detect early to determine hair transplant candidacy and guide treatment options

Diagnosing Hair Loss: It’s More Than Just Looking at Your Scalp
Hair loss is often more complex than it appears. It’s not just about noticing extra hairs in the shower or thinning areas. Diagnosing the cause requires a thoughtful and comprehensive approach, reviewing your hair loss history, examining your scalp and hair, and assessing your health history, nutrition, blood work, and lifestyle factors.
At YAKER Hair Restoration + Med Spa, we don’t just treat symptoms — we find the why.
A 360-Degree Approach
A proper evaluation includes:
- Hair loss history: timeline and pattern of hair loss
- AI-powered scalp analysis with TrichoLab for precise imaging
- Review of medical & family history
- Review of medications, supplements, diet, hair care products, and practices
- Lifestyle factors (diet, stress, sleep, etc.)
- Comprehensive blood testing
What If It’s Not Genetic Hair Loss?
Not all hair loss is caused by genetics. When there’s sudden, patchy, or widespread shedding, we dig deeper.
Other causes we consider:
- Telogen effluvium (TE): Triggered by stress, illness, nutritional or hormonal imbalances, and scalp or systemic inflammation
- Diffuse alopecia areata: Autoimmune-related hair loss
- Cicatricial (scarring) alopecia: Inflammation that permanently damages hair follicles
These conditions often overlap, making it difficult to determine what is truly happening. That’s why a thorough evaluation matters.
When men notice thinning hair, it’s often a sign of more than hair issues—it can hint at deeper health changes. Let’s explore the hidden causes—and what you can do about them.
Hair Loss Isn’t Always Just About Hair
What’s Happening Inside: Hidden Health Links to Hair Loss
When most people think of hair loss, they assume it’s only a cosmetic issue. But androgenetic alopecia (AGA)—also known as male pattern baldness—is more than a hair issue. Research shows it can be connected to other health problems that share similar genetic, hormonal, or metabolic roots.
Cardiovascular Disease
Men with AGA—especially early onset—are more likely to develop heart conditions like:
- High blood pressure (hypertension)
- Coronary artery disease (CAD)
Why the connection?
- Androgen sensitivity genes may affect both hair follicles and blood vessels
- DHT can impair vascular function and increase bad cholesterol
- Chronic inflammation and oxidative stress, common in both AGA and heart disease, damage blood vessels and hair follicles alike
- Men who start balding before age 30 may face a higher risk of serious cardiovascular disease later in life
Metabolic Syndrome
This cluster of conditions includes: 2
- Obesity
- High blood pressure
- Insulin resistance
- Abnormal cholesterol
Men with AGA are more likely to develop metabolic syndrome, which increases heart disease risk.
Why?
Androgen (male hormone) sensitivity, insulin resistance, and low-grade inflammation affect both metabolism and hair loss progression.
Insulin Resistance & Type 2 Diabetes
AGA has been associated with insulin resistance and blood sugar dysregulation. 3 4
- Decrease blood flow to the scalp
- Increase DHT activity
- Promote inflammation and follicle damage
This can speed up the miniaturization process in genetically susceptible individuals.
Benign Prostatic Hyperplasia (BPH)
DHT plays a major role in both: 5 6
- AGA, by shrinking hair follicles
- BPH, by enlarging the prostate
Men with AGA may be at a higher risk of developing urinary symptoms due to an enlarged prostate as they age.
Mental & Emotional Health
Hair loss isn’t just physical—it affects how people feel:
- Self-esteem drops as the hairline recedes
- Anxiety or depression is common, especially with early or aggressive AGA
- Body image issues can impact relationships, career confidence, and quality of life
Mental health support is just as important as medical treatment in many cases.
Sleep Disorders
Some studies suggest men with AGA may be more likely to experience disrupted sleep quality 7 or obstructive sleep apnea (OSA). 8
Why?
- Shared traits, such as obesity, metabolic disorders, and inflammation, may be linked to the two
- OSA affects hormone balance and blood flow—both crucial for healthy hair growth
What This Means for You
AGA might start at the scalp—but its reach can go far beyond hair.
If you’re dealing with significant or early-onset hair loss, it’s worth having a broader health check-up.
Ask your provider about:
- Heart health screening
- Metabolic panel (glucose, lipids, insulin)
- Inflammation markers
- Sleep apnea evaluation if you have sleep issues
- Prostate health (if you’re over 40)
What Makes Male Pattern Baldness Worse?
Hidden Triggers of Androgenetic Alopecia (AGA)
Testosterone Therapy: A Double-Edged Sword
Testosterone therapy is on the rise—yet many men start it without needing it, or without proper testing or follow-up. Studies show:
- Many men take testosterone without needing it
- 1 in 4 men begin testosterone therapy without checking hormone levels first.
- Nearly half aren’t monitored appropriately after starting.
- They are given ultra-high doses unnecessarily to get you hooked and keep coming back
- They are convinced that the cause of all their problems is “low” testosterone
That’s a problem.
Free vs. Total Testosterone: Know the Difference
Free testosterone is the active form your body uses to regulate libido, muscle growth, mood—and yes, hair loss.
It’s also the form that gets converted into DHT, the main driver of AGA.
Too many clinics focus on total testosterone levels without ever measuring free testosterone, which is what really matters when it comes to treating low testosterone and minimizing hair loss risk.
How DHT Sensitivity Accelerates Hair Loss
Everyone makes DHT, but not everyone’s hair reacts the same.
- If you’re genetically sensitive, even normal levels of DHT can trigger hair loss
- If you’re not genetically sensitive, you might have high testosterone and still keep your hair
The key isn’t just how much testosterone you have—it’s how your follicles respond to it. That’s why pushing testosterone too high (even for “anti-aging” reasons) can speed up balding in vulnerable patients.
Optimal Testosterone Levels by Age
With the growing popularity of testosterone replacement therapy (TRT), I regularly see men and women seeking help for hair loss concerns. Alarmingly, 90% of these patients have testosterone levels well above the normal range for their age. More than 65% do not have their hormone levels monitored regularly, and 95% fail to test free testosterone.
For men, testosterone levels generally peak at age 30 and gradually decline with age. All testosterone values can vary slightly between laboratories, but here’s a general guide:
| Age | Total Testosterone Range | Avg. Total T | Free Testosterone Range | Avg. Free T |
|---|---|---|---|---|
| 19–29 | 264–916 ng/dL | ~600 ng/dL | 9.3–26.5 ng/dL (93–265 pg/mL) | ~15 ng/dL (150 pg/mL) |
| 30–39 | 264–916 ng/dL | ~600 ng/dL | 8.7–25.1 ng/dL (87–251 pg/mL) | ~14 ng/dL (140 pg/mL) |
| 40–49 | 250–850 ng/dL | ~550 ng/dL | 6.8–21.5 ng/dL (68–215 pg/mL) | ~12 ng/dL (120 pg/mL) |
| 50–59 | 215–850 ng/dL | ~500 ng/dL | 6.1–19.3 ng/dL (61–193 pg/mL) | ~10 ng/dL (100 pg/mL) |
| 60–69 | 196–859 ng/dL | ~450 ng/dL | 5.0–16.7 ng/dL (50–167 pg/mL) | ~9 ng/dL (90 pg/mL) |
| 70+ | 156–819 ng/dL | ~400 ng/dL | 4.5–13.9 ng/dL (45–139 pg/mL) | ~8 ng/dL (80 pg/mL) |
Aim to keep your free testosterone in the average range for your age—not above it. Ensure labs include free testosterone, not just total levels.
Going too high cannot only increase your chances of experiencing more hair loss but also lead to other unwanted side effects.
The Dark Side of High Testosterone: What Every Man Should Know
When testosterone levels climb too high—especially without proper monitoring—it can lead to serious, sometimes irreversible side effects.
Hormone Imbalances
- Estrogen conversion → gynecomastia (male breast enlargement)
- Suppressed natural testosterone → infertility, testicular shrinkage
Heart & Metabolic Risk
- Polycythemia → thickened blood, leading to increased blood clot, heart attack, and stroke risk
- Increased LDL, decreased HDL → heart disease
- Insulin resistance → poor blood sugar control→ higher chance of developing type 2 diabetes
Liver & Kidney Strain
- Potential liver toxicity and impaired kidney function
Mood & Behavior
- Aggression, irritability, anxiety, or depression
Skin & Hair
- Oily skin and acne breakouts
- Accelerated hair loss in genetically prone individuals
- Worsening scalp seborrheic dermatitis (due to increased sebum production)
Prostate
- BPH (enlarged prostate) → urinary symptoms
Can Testosterone Trigger Hair Loss—Even with Using Hair Treatments?
Yes—and here’s why.
If you’re using DHT blockers (like finasteride/dutasteride) but still losing hair on testosterone, this might explain it:
Think of it like blood pressure meds—you can’t eat high-sodium foods and expect the pill to work.
Similarly, if you’re increasing DHT with high testosterone, it can overpower the meds trying to reduce it.
Why Hormone Clinics Often Miss the Hair-Loss Connection
When you see a hormone specialist to optimize your testosterone, hair loss may not even come up. That’s because:
Genetics Aren’t on Their Radar
Hormone doctors focus on lab numbers—not hair loss history. But if you have the genes for male pattern hair loss, your follicles react more strongly to DHT (a byproduct of free testosterone).
Final Thoughts on Testosterone
If you’re concerned about hair loss while on testosterone therapy:
- Let your hormone specialist know about your hair loss
- Stay within age-appropriate ranges—check your free testosterone range with your hormone specialist to ensure they don’t go too high
- Get your free testosterone checked regularly—not just total testosterone
- Avoid chain clinics that follow a one-size-fits-all approach
- Combine therapy with proper DHT-blocking treatments
Insulin Resistance and Hair Loss
Insulin resistance or diabetes can worsen genetic hair loss by:
- Increasing free testosterone → more DHT conversion
- Reducing blood flow to the scalp → fewer nutrients to the hair follicles
- Promoting inflammation and oxidative stress → damaged hair follicles
The fix: Control blood sugar, improve circulation, reduce inflammation, and address hormone balance.
The Smart Way to Treat Hair Loss
Treating AGA effectively means looking at the entire picture—including your hair loss history, overall health, blood work, and lifestyle.
These details help build the most effective strategy for slowing or stopping the loss and improving hair density.
FDA-Approved Treatments
- Topical Minoxidil
- Boosts blood flow to follicles
- Helps maintain density and slow shedding
- Oral Finasteride
- Reduces DHT to prevent further hair follicle miniaturization
- Slows progression and can help rethicken miniaturized hair
Other Promising Off-Label Treatments Include:
- Topical Finasteride
- Oral and topical Dutasteride
- Oral Minoxidil
- Low Level Laser Therapy (LLLT)
- Platelet rich plasma (PRP) injections
- Nutritional support targeting inflammation and oxidative stress
These therapies can help slow the progression of hair loss and improve hair thickness. However, they cannot regrow hair in fully bald areas, and results are not permanent—if you stop treatment, most gains fade within 6–12 months.
Why Starting Early Matters
AGA is a progressive condition, meaning it gets worse with age. Once hair follicles miniaturize beyond a certain point, they become unresponsive—even to the best treatments.
- Start early
- Stay consistent
- Avoid treatments that are not backed by sound science
- Pair medical and lifestyle interventions

